
Human vs AI Medical Scribes in Healthcare: When Each Makes Sense
The honest answer to human scribe vs AI scribe isn't universal. It depends on your environment, your billing complexity, and what failure modes your department can and can't afford. Here's how to think through it clearly.

Emergency departments run on documentation. Every patient encounter, every clinical decision, every billing level depends on how well that documentation gets done - and who, or what, is doing it. The question of whether to use human scribes, AI scribes, or some combination of both is one more ED administrators are facing right now, and the answer isn't as straightforward as most vendor pitches make it sound.
The Question Every ED Administrator Eventually Faces
It's a Friday night. Your busiest shift of the week. And the human scribe who was supposed to be in at 7pm just called out sick.
The attending is now documenting solo, typing between patients, finishing charts after midnight, trying to remember the specifics of encounter fourteen while managing encounter twenty-two. By the end of the shift, documentation quality has slipped, notes are thinner than they should be, and there's a reasonable chance that several charts won't support the billing level the clinical care actually justified.
Or maybe you're on the other side of this scenario entirely. You've just sat through a polished AI scribe demo, the numbers look compelling, and now you're trying to figure out whether what you saw in a controlled presentation will actually hold up in the controlled chaos of a real emergency department.
Both situations lead to the same question: human scribe or AI scribe, which one actually works in an ED?
The honest answer is that it depends. It depends on your volume, your billing complexity, your staffing reality, and what problem you're primarily trying to solve. This article is written specifically for emergency medicine administrators, medical directors, and CFOs working through that decision. Not for primary care, not for outpatient clinics, but for the specific conditions that make the ED one of the most demanding documentation environments in healthcare. The comparison looks different here than it does anywhere else in the hospital, and it's worth understanding exactly why before making a call in either direction.
What You're Actually Comparing
Before getting into strengths and weaknesses, it helps to be precise about what each option actually looks like in a working emergency department, not in a brochure.
A human scribe in an ED is typically a trained documentation assistant who follows a physician through their shift, either physically present in the room or connected via audio and video. They listen to the encounter, document the note in real time, and submit it for physician review and sign-off. Their effectiveness depends heavily on their training level, their familiarity with emergency medicine clinical vocabulary, and their individual consistency from one shift to the next.
An AI scribe is an ambient or voice-activated platform that listens to the patient encounter and automatically generates a structured clinical note. The physician reviews, edits if needed, and signs off. No human intermediary, no staffing dependency, no coverage gaps.
At a surface level, the two options are doing the same job: capturing what happens in a patient encounter and turning it into a documented clinical record. But the way they do it and the failure modes they carry are meaningfully different.
There's also a variable that makes this comparison uniquely high-stakes in emergency medicine specifically: MDM billing complexity. Since 2023, ED evaluation and management coding is determined entirely by Medical Decision Making complexity, a shift that reshaped how every emergency department in the country should be thinking about documentation. A note that accurately reflects the clinical complexity of an encounter bills at a higher level than a note that doesn't, even if the care delivered was identical. That means every documentation gap, every inconsistency, every missed element has a direct financial consequence. Any scribe solution, human or AI, has to be evaluated with that reality as the baseline.
Where Human Scribes Still Have a Genuine Edge
A fair comparison starts with honest acknowledgment of where human scribes actually perform well. There are real scenarios where a trained human scribe outperforms current AI tools, and dismissing that doesn't serve anyone making this decision.
✦ Real-Time Adaptability: Trained human scribes can follow the non-linear flow of an ED encounter, picking up on contextual cues and adjusting documentation in the moment. Current AI tools are improving here, but experienced scribes still handle conversational complexity with a fluency that ambient AI doesn't always match.
✦ High-Chaos Scenarios: In active resuscitations and trauma activations, experienced scribes can filter signal from noise in ways that remain genuinely difficult to replicate programmatically.
✦ Established Physician Relationships: A scribe who has worked alongside the same attending for years develops a documentation shorthand that functions almost as an extension of the physician's own workflow. That kind of embedded trust doesn't transfer overnight to a new tool.
The honest conclusion: human scribes are a legitimate solution with real strengths, particularly in high-acuity environments and in departments where physician adoption of new technology is a significant cultural variable. None of what follows is meant to dismiss that.
Where Human Scribes Create Operational Risk
With that said, human scribing in emergency medicine carries a set of structural vulnerabilities that become harder to ignore the longer a department runs on them. These aren't edge cases. They're the predictable failure modes of a staffing-dependent documentation model applied to a high-volume, 24/7 environment.
1. Availability and Coverage Gaps
Human scribes call out sick, leave for graduate school, have family emergencies, and simply aren't available at 3am during a surge. Every gap in scribe coverage is a gap in documentation quality, and unlike a missed shift in most hospital roles, a missed scribe shift means the physician absorbs the documentation burden directly, in real time, during patient care. There is no redundancy built into a human scribing model unless you're paying for it explicitly through overstaffing.
2. Inconsistent Documentation Quality
Even in a well-run scribing program, note quality varies by individual. It varies by how long a scribe has been with the department, by how much clinical training they have, and honestly by how tired they are at hour nine of a shift. Two scribes documenting the same encounter type can produce charts that support different billing levels, not because the care was different, but because one understood MDM complexity better than the other. That inconsistency is invisible until an audit or a revenue cycle review surfaces it.
3. Training Overhead and Ramp Time
A new human scribe typically takes four to eight weeks to reach a documentation level that reliably supports accurate billing. During that window, physicians spend meaningful time correcting and supplementing notes rather than trusting them, which defeats much of the efficiency value the scribe is supposed to provide. Healthcare support staff turnover runs well above 30% annually in many settings, meaning that ramp cycle repeats far more often than most administrators budget for.
4. Scaling Cost
Human scribing is a per-head expense. Every additional provider, every extended coverage window, every new shift added to the schedule requires an additional hire. There is no volume efficiency, and cost scales linearly with need, which makes human scribing increasingly difficult to justify financially as departments grow or patient volumes rise.
None of these are reasons to eliminate human scribing categorically. But they are reasons to take the operational math seriously before assuming that the current arrangement is the safe or neutral choice.
Where AI Scribes Perform Strongest - And Where They Fall Short
"AI scribing in emergency medicine has matured considerably over the past few years, and the distinction between purpose-built ED platforms and general-purpose tools has never been more pronounced."
Where AI Scribing Performs Strongest in an ED Context
The best AI scribe platforms built for emergency medicine don't just solve the problems human scribes create - they introduce capabilities that a staffing-dependent model structurally cannot offer. These are the areas where that difference shows up most clearly in day-to-day ED operations.
✦ Consistency at Volume: An AI scribe doesn't have a bad shift. The note generated at encounter thirty-eight of a busy Saturday night is structurally identical to the note generated at encounter two. For departments where billing accuracy is a priority, and in emergency medicine it always should be, that consistency has direct revenue implications that compound across every shift, every month, every year.
✦ Availability without Exception: No call-outs, no coverage gaps, no staffing math. An AI scribe performs at the same level at 2am on a holiday as it does at 10am on a Tuesday. For EDs running 24/7 with no natural slow period, that reliability is operationally significant in a way that's difficult to overstate.
✦ Scalable Cost Structure: Once an AI scribing platform is in place, the marginal cost of an additional provider using it is minimal compared to hiring an additional human scribe. For growing departments or health systems managing multiple ED locations, this structural difference becomes a meaningful financial advantage over time.
MDM billing analysis: This is where the strongest ED-specific AI scribe platforms separate themselves most clearly, not just from human scribes, but from general-purpose AI scribing tools. Purpose-built platforms don't just transcribe the encounter. They analyze whether the documented clinical content supports the appropriate MDM billing level and flag discrepancies before a chart is submitted. No human scribe, regardless of training level, is performing that analysis in real time on every note.
Where AI Scribes Fall Short
Applying the same honest lens here matters, because not every limitation is a dealbreaker and not every AI scribe handles these gaps the same way. These are the areas worth pressure-testing before committing to any platform.
1. Audio Environment Sensitivity
In the most chaotic ED scenarios, with simultaneous voices, equipment alarms, and rapid-fire interventions, some AI platforms still struggle with transcription accuracy. This gap is narrowing quickly as the technology matures, but it remains a real variable depending on the platform and the specific environment.
2. Physician Adoption
Some attending doctors, particularly those who have documented the same way for years, resist changing their workflow for a new tool. Adoption is a real implementation variable, and a platform that physicians don't trust or use consistently doesn't deliver its theoretical ROI regardless of how well it performs technically. New research found that documentation support tools only produced meaningful time savings for physicians who adopted them at high intensity, a finding that underscores how critical real-world adoption is to any projected return.
3. Not all AI Scribe Tools are Built for Emergency Medicine
This is the most important caveat in this entire article. A general-purpose AI scribe designed for outpatient primary care or specialist visits often lacks the ED-specific clinical vocabulary, the MDM billing analysis layer, and the workflow design that emergency medicine actually demands. Applying the wrong AI scribe to an ED can produce the same documentation inconsistency problems as an undertrained human scribe, just faster and at greater scale.
Real Comparison - A Framework for Your ED
With both options evaluated on their actual merits, the decision comes down to six variables that should drive the choice in any emergency department, regardless of size, system affiliation, or current setup.
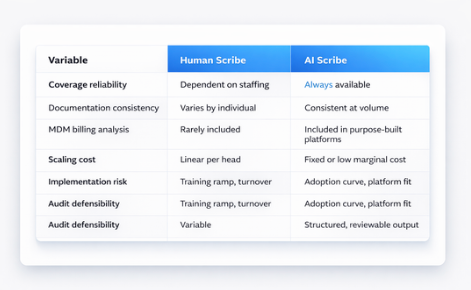
The table makes the structural differences clear, but for most emergency departments the deciding row is the third one. MDM billing analysis is the variable that separates a documentation solution from a revenue solution. If your current scribe setup, human or AI, is not actively reviewing whether your charts support the billing level your clinical care justifies, documentation efficiency is only solving half the problem. The revenue leakage continues regardless of how fast the notes get done.
That's the finding that anchors the DocAssistant AI case study with Elite Hospital Partners: $399,000 recovered per provider per year in previously lost revenue. Not from seeing more patients, not from reducing overhead, but from ensuring that the clinical care already being delivered was documented and billed at the level it actually supported. The full picture behind those numbers is worth reviewing if you're building a business case internally.
When to Keep Human Scribes, When to Transition, and When to Combine
The right answer for your department depends on where you sit across the variables above. Here's a practical breakdown.
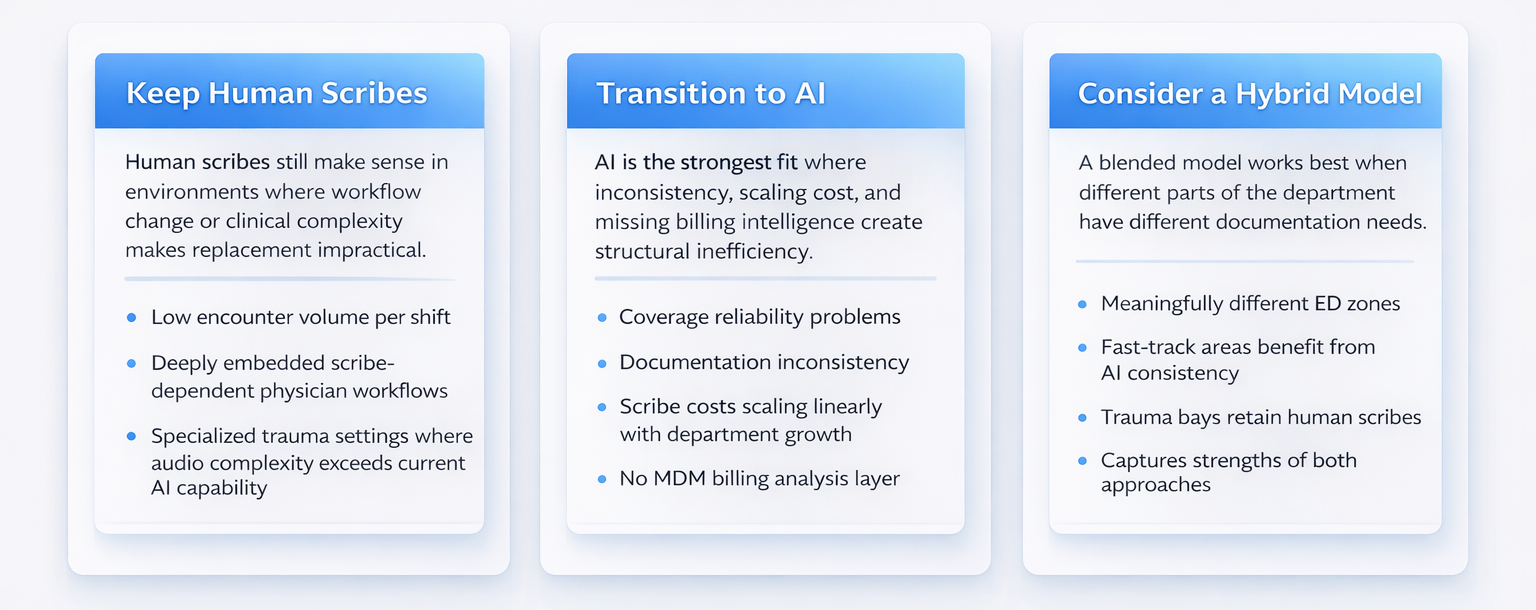
Keep Human Scribes If:
- Your department runs a relatively low volume of encounters per shift
- Physicians have deeply embedded scribe-dependent workflows requiring significant cultural change
- You're in a specialized trauma environment where audio complexity exceeds current AI capability
Human scribes in these contexts deliver real value, and the disruption of switching may not be justified by the return.
Transition to AI If:
- You're experiencing coverage reliability problems or documentation inconsistency
- Scribe costs are scaling linearly with department growth
- Your current setup has no MDM billing analysis layer
These are the conditions where purpose-built AI scribing delivers measurable, near-term ROI that a human scribing model structurally cannot match.
Consider a Hybrid Model If:
- Your ED has meaningfully different zones with different documentation demands
- High-volume fast-track areas could benefit from AI consistency while trauma bays retain human scribes
That kind of thoughtful deployment captures the strengths of both approaches rather than forcing a single solution onto every corner of the department.
Why DocAssistant AI Was Built for This Specific Decision
Most of the limitations identified in the AI scribe column above trace back to a single root cause: general-purpose tools being applied to an environment they weren't designed for.
Emergency medicine has documentation demands that are fundamentally different from the rest of the hospital. The volume is higher, the encounter types are more varied, the billing complexity is greater, and the consequences of documentation gaps are more immediate. A tool designed for a primary care visit or a specialist follow-up is not equipped to handle that environment at the level emergency departments actually need.
DocAssistant AI was built specifically for ED environments, and that specificity shows up in three concrete ways that map directly to the framework above.
The MDM billing analyzer is integrated into the documentation workflow, not bolted on as an afterthought. Every chart is reviewed against the 2023 CMS E/M guidelines in real time, and undercoding is flagged before submission. Physicians don't have to think about billing level optimization while managing patient care. The platform handles it.
The system is EHR-agnostic, integrating with existing infrastructure rather than requiring a system change or a new vendor relationship. That means implementation doesn't create EHR lock-in risk, and your documentation capability isn't held hostage to a single platform contract.
DocAssistant AI holds SOC 2 Type 2 certification, meaning its data handling and security architecture has been independently verified. In a post-2023 MDM coding environment where audit exposure is a real operational risk, that certification is a defensible answer to the question your compliance team will eventually ask.
The outcome at Elite Hospital Partners speaks to all of this directly:
$399,000 recovered per provider per year in previously lost revenue.
Those numbers came from a real ED implementation, not a demo environment, not a pilot with hand-selected cases, but a working emergency department running the platform across its standard patient volume.
For anyone still weighing what that translates to in practice, the documentation errors that drive this level of revenue loss are more common and more preventable than most departments realize until they look closely.
For context on what that looks like against the cost of human scribing: a full-time human scribe typically runs between $35,000 and $55,000 per year in salary and benefits, covers one provider during one shift, and includes no billing analysis. At $399,000 in recovered revenue per provider, the financial comparison is not particularly close.
Making the Case Internally
If you're the person in your organization who has worked through this analysis and now needs to bring leadership to the same conclusion, the argument distills to this:
The question is not whether AI scribes are better than human scribes in the abstract. The question is whether your current documentation setup, whatever form it takes, is capturing the revenue your clinical care actually justifies. If it isn't, the gap between what you're billing and what you could be billing is a predictable, measurable number. And closing it is a defensible decision, because the data exists to support it.
The risk of staying with the status quo is not neutrality. Every shift that runs on a documentation model without MDM billing analysis is a shift where revenue leaks out invisibly. That compounds over months and years in ways that are surprisingly large when finally quantified, and surprisingly straightforward to address once the right tool is in place.
The Bottom Line
Back to that Friday night scenario. The attending documenting solo after a scribe call-out, or the administrator trying to evaluate a vendor demo with no clear framework for comparison. Both situations have the same underlying answer: the right documentation solution is the one that shows up reliably, documents consistently, and captures the billing level your clinical care supports, every shift, not just when conditions are ideal.
Human scribes can be the right answer in the right environment. But in a high-volume emergency department where MDM billing complexity is real and revenue recovery matters, the structural limitations of a staffing-dependent documentation model are difficult to overcome. The math tends to resolve clearly once all the variables are on the table.
If you're currently evaluating AI scribes or weighing a transition away from human scribing, DocAssistant AI offers structured pilots designed specifically for ED environments, including a billing analysis review that shows you exactly what your current documentation setup is leaving on the table. No commitment required to see the numbers.
About DocAssistant
DocAssistant develops HIPAA-compliant AI documentation and medical coding solutions purpose-built for emergency medicine. Founded by practicing emergency physicians and headquartered in San Diego, California, DocAssistant combines automated clinical documentation with specialty-specific AI to reduce documentation burden, improve ICD-10 coding accuracy, and increase revenue capture for physicians, billing teams, and healthcare organizations. The company’s AI coding tool and AI scribe platform are designed to help medical billing teams, revenue cycle professionals, and clinicians work faster and document more completely. More information is available at www.docassistant.ai.
Media Contact:
DocAssistant Team
+1 619-344-0849


